
A. Introduction
The virus that causes Covid-19 has struck countries around the world, and it is the same virus everywhere. But countries have responded differently. Many countries have responded effectively, and some highly effectively. The US is not among them. The experience in other countries shows what would have been possible, had the US responded as they did. Unfortunately, the US, with Trump leading as president, did not.
B. The US Compared to Italy, Spain, Germany, and the UK
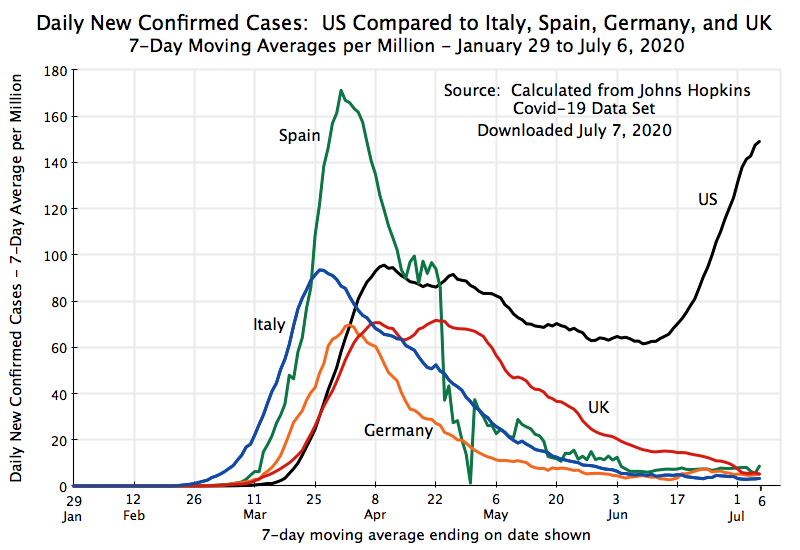
The chart above shows the daily number of new confirmed cases (on a 7-day moving average basis) since the start of the pandemic through to July 6, for the US plus several of the larger countries of Western Europe: Italy, Spain, Germany, and the UK. These countries were chosen in part as they were all hit with the virus that causes Covid-19 earlier than most (including earlier than in the US). They thus faced a crisis when much was still not known about the virus, including how quickly it could spread and under what conditions, and uncertainty on what should be done to bring it under control. The underlying data on Covid-19 case totals, from which the figures for the chart were derived, comes from the widely-used data set maintained by Johns Hopkins University. Population numbers from the UN were used to put the number of cases on comparable terms: of daily new cases per million residents.
Italy was the first major country in Europe to have been hit by the virus, for reasons still not fully known. Cases rose quickly, reaching a peak at the end of March. Spain came next, roughly a week later than Italy at first, but then rose especially quickly to a peak in early April of almost double the peak in Italy. Germany also had a high number of cases early, but was then more successful through aggressive testing and quarantining to keep the peak from rising as high. Finally, the UK saw a similar peak to that of Germany, but with that peak then lasting for close to a month.
Each of these European countries was then able to bring their daily new case numbers down sharply, to less than 10 new cases a day per million residents by early July (and indeed by early June for all other than the UK). Each country had its own policies, and I will not go into the nuances of the country-specific differences here, but they succeeded through a combination of social distancing (including lockdowns), wide use of masks, extensive testing, contact tracing, and then isolation or quarantining of those infected or exposed to someone infected. And with their success in bringing down the number of Covid-19 cases, these countries are now opening up for business, schools, and travel, and are doing so safely.
The US followed a different path. Cases rose similarly at first as in these European countries, although with a lag (or about two weeks compared to Italy). One should be cautious with these early numbers as testing, particularly in the US, was not as complete as was being done later, but the early trends appear to be broadly similar.
But what is important is what happened next. In contrast to the European countries, who were all able to bring down their case numbers by 90% or more, new daily cases in the US fell much more modestly. Despite official policies (in much, although not all, of the country) to lock down the economy to limit person-to-person spread of the virus, plus guidelines encouraging (and in some cases mandating, but with lax to no enforcement) the wearing of masks and social distancing, the daily case numbers in the US were reduced only from about 95 per million in early/mid April to a trough in early June that never fell below 60.
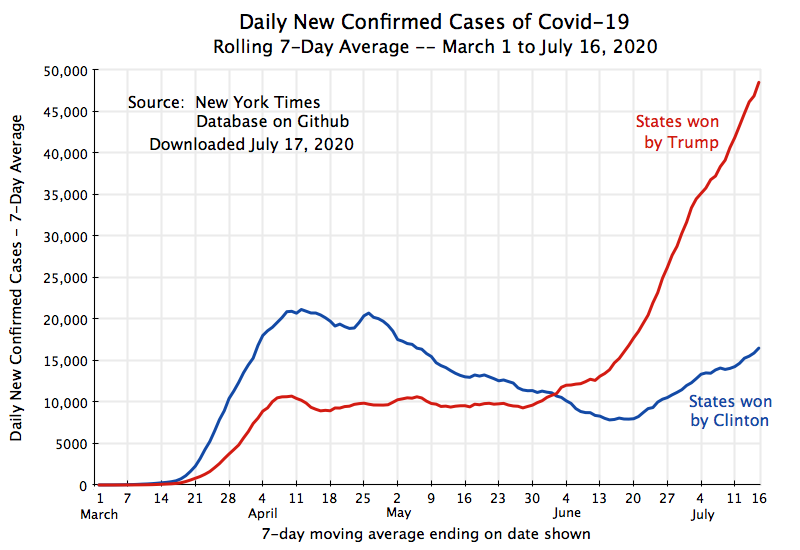
US cases then started to shoot up. This followed the easing of social distancing and other measures to limit the spread of the virus during the month of May. While there were important differences by state and indeed often by locality, most states started to lift the measures cautiously in early May and much more comprehensively by the end of May (and sometimes completely so by that point). And as was examined in an earlier post on this blog, the increases in daily cases have been particularly sharp in the states won by Trump in 2016 – states often with governments and a population that have been particularly aggressive in lifting (or increasingly ignoring) those measures.
As a further example of the impact of this politicization of what should be seen as basic public health measures, the number of Covid-19 cases in Tulsa, Oklahoma, have now spiked two weeks after Trump held a large campaign rally in an indoor arena there. Local health officials have said it is “more than likely” that the two are linked. Few at the Trump rally wore masks, they were grouped closely together for the cameras, and loud cheering was of course encouraged. The two week lag from the rally to the spike in Covid-19 cases is about what health experts say one should expect, between when there is exposure to the virus at an event such as this to when confirmed case numbers will rise as results are obtained for people seeking tests following an onset of symptoms.
C. The US Compared to Europe, Canada, and Sweden
The chart at the top of this post highlights only a few countries. But the same results hold for Western Europe as a whole as well as for Canada:

Cases in Western Europe as a whole rose early, reached a peak, and then fell. Since early June cases have remained below 10 per day per million. As of July 6, they were at 8.3, or less than 6% of the US rate of 149 per day. The path for the countries of Eastern Europe (the countries from Estonia on the north to Bulgaria on the south, who are now mostly members of the EU) is interesting as they were able to contain the virus throughout, with a peak of less than 14 in early to mid-April. But a modest increase in recent weeks (to almost 15 currently) warrants watching.
Canada is also interesting as the economy and the population are broadly similar to that of the US, but with very different politics. Cases rose in Canada to a peak of about 50 in mid-April. But they were then brought down, to levels now very similar to that of Western Europe. Again, this is in sharp contrast to the US.
Sweden is an exception to others in Europe. It is also the one country of the rich Western democracies that explicitly followed a different policy path. Instead of mandating a lockdown of the economy, the wearing of masks, social distancing, and other such measures, it only issued general guidance. And even this guidance was eased later. Daily cases per million then reached about 60 in late April, fell only modestly to about 50 in late May, before increasing significantly to as much as 120 at points in June (although with erratic numbers that probably reflect reporting practices). Sweden is now taken as a good example of what not to do. Furthermore, while “protecting the economy” was presented as a rationale for Sweden’s decision to issue only general guidelines, with no requirement for businesses such as restaurants to close, early evidence indicates that the Swedish economy has suffered similarly to those of its neighbors. There was no economic gain, but a profound human loss in sickness as well as lives. As I write this (July 9), the accumulated number of deaths per million of population has come to 545 in Sweden, or roughly ten times the totals of 46 in neighboring Norway and 59 in Finland.
D. The US Compared to East Asia, Australia, and New Zealand
Europe (with the exception of Sweden), as well as Canada, have therefore been far more successful than the US in limiting the spread of the virus that causes Covid-19. But the countries that have been by far the most successful in containing the virus have been those of East Asia, as well as Australia and New Zealand:

Drawn on the same scale as the other charts, one can barely distinguish their case levels, other than during a few, and still always low, periods (in early March in South Korea and in late March and early April for most of the others). And the daily case rates in Taiwan were never over 1 per million of population, so one cannot distinguish its curve from the horizontal axis of the chart. Yet Taiwan has probably closer contact with China, from business relationships as well as personal travel, than any other country in the world other than Hong Kong.
All of these countries reacted quickly as soon as it became clear that an infectious disease had spread in China. While travel limits were imposed, these limits were complemented by extensive testing and contact tracing, quarantining of all travelers (whether citizens or not), and wide use of masks and other social distancing measures. None of this was secret. Nor did it require special expertise. Others could have responded similarly, but did not.
E. Countries with a Similar Result as the US
Which, then, are the country cases that are broadly comparable to that of the US? The closest are Brazil and South Africa, with similarities also in the cases of Russia and Mexico:

These are not countries that the US would normally compare itself to. One should certainly be cautious and note that the quality of the case number data may not be all that good in some of these countries (and indeed, it is not all that good in the US itself). But the patterns are probably broadly accurate.
Brazil is the one major country in the world with more confirmed cases (per million of population) than the US. Its right-wing president, Jair Bolsonaro, has responded to the virus in many ways similar to Trump. He has consistently downplayed the virus (like Trump), has refused to wear a mask (like Trump), has encouraged rallies to oppose rules on social distancing that some Brazilian states and localities had issued (also like Trump), and has insisted that the disease is not serious but rather “It’s just a little flu or the sniffles”. And like Trump, he accuses the media of stoking hysteria.
The result is that the number of cases in Brazil per million of population is now the highest of any large country in the world, and indeed second only to the US in absolute total number. And on July 7, Bolsonaro himself tested positive for the virus. Again like Trump (who took the drug when he was possibly exposed to the virus), Bolsonaro is now taking doses of hydroxychloroquine as a treatment, even though there is clear evidence that this drug does not help with Covid-19 and may in fact do harm.
Other countries with rising numbers of new cases include South Africa and Mexico. The daily cases for South Africa now match the US number, with a path since mid-June broadly similar to the US path. Russia saw an increase in April to mid-May, after which there has been some decrease. But the daily numbers in Russia remain high.
F. Conclusion
There is not much here for the US to be proud of. While countries in Western Europe, as well as Canada, saw sharp increases in cases in much of March and early April, they were then all (with the notable exception of Sweden) able to bring the rates for new cases down to modest levels. With that success, they are now reopening their economies, are permitting travel (other than, notably, to and from the US), and will be reopening schools. They are all still cautious, and maintain aggressive efforts at testing, contact tracing, and then quarantining when warranted, but their success in bringing down the daily case numbers means they can, albeit carefully, resume a degree of normalcy. It is possible that things will take a turn for the worse in the weeks and months ahead. Until there is an effective vaccine that is broadly available, there will remain conditions in which the virus could pop up and cause major disruptions again. But the situation in these countries has remained stable there for more than a month now.
Countries in East Asia, as well as Australia and New Zealand, have done far better. They kept rates low from the start and have thus been able to reopen safely and more quickly. Indeed, schools in Taiwan never even closed (other than for a two-week extension of the traditional Chinese New Year holiday in February). But Taiwan then opened schools safely, with students required to wear masks, temperature checks carried out daily of all students, and with plastic shields installed to separate desks from each other. [Not everyone liked this. I know from direct personal information that at least a few elementary school age children thought it horribly unfair that they have had to go to school while children around the world were able to stay home.]
So who resembles the US in effectiveness in limiting the spread of the virus that causes Covid-19?: Among the larger countries of the world, only Brazil and South Africa, and to some extent Mexico and Russia. In the past, they were not the countries the US would see as comparables. But they are now.






You must be logged in to post a comment.